This year, the AIDS crisis will turn 30, a testament not only to the epidemic’s resilience but also to a global movement’s long struggle for visibility and survival. There’s no debating that in those three decades, domestic and global efforts to stem the spread of HIV/AIDS made major strides. But activists say that efforts have slumped lately, and the U.S. is failing in its traditional role at the helm of the international response.
The Obama administration has taken an "integrated" approach to addressing HIV/AIDS through its Global Health Initiative, which tackles many health issues that often compound each other: HIV, infant and maternal health, malaria, tuberculosis, health systems and health workforce; as well as neglected tropical diseases.
That strategy was hailed initially by many global health watchdogs, who have long said that HIV can’t be addressed in a vacuum. But at least one group now says the more expansive strategy has camouflaged the shortchanging of HIV/AIDS programs.
Obama’s fiscal year 2011 budget proposal inched up HIV/AIDS funding under the Global Health Initiative by 3.5 percent, according to the Kaiser Family Foundation; Congress has not yet passed that budget. But according to Health Global Access Project (GAP), which advocates for HIV/AIDS funding worldwide, funding has effectively plateaued or even retrenched during Obama’s first two years in office. The group says Obama’s policies could undermine the progress made under the President’s Emergency Plan for AIDS Relief (PEPFAR), a Bush-era initiative that marshaled U.S. and international money to invest in treatment and prevention in high-risk regions.
According to GAP’s analysis of PEPFAR spending, 2010 saw a 14 percent decrease from the previous year in the the anti-retroviral drug budget, as well as significant cuts in several country-specific programs in Africa. The group blasted the administration for "flat-lining the response to AIDS" and "decreasing investments in essential program areas for the first time since PEPFAR was funded."
Ezekiel Emanuel, head of Obama’s Global Health Initiative, put a positive spin on economizing the AIDS budget. Stressing that "what counts are not dollars spent or drugs bought, but lives saved," he argued in the Huffington Post:
What it takes to save lives of those with HIV and those most at risk to contract it is a comprehensive approach that recognizes the roles of other diseases (many inexpensively preventable), child and maternal health, and strong health systems play in saving lives and solidifying health gains in developing nations.
While a more holistic approach to global health is vital, AIDS activist Gregg Gonsalves wrote in the Washington Post, dollars do matter when it comes to fighting a virus as brutal as HIV:
AIDS activists have been global health activists all along, with many calling for health-care reform in the United States since the epidemic first appeared and for strengthening primary care in the developing world for more than a decade. What we don’t support is this administration’s either/or approach to global health.
Whether funding rises or falls in the upcoming federal budget, there will still be a yawning global gap in treatment and prevention resources, especially in the hard-hit African nations that had been a major recipient of PEPFAR dollars. According to UNAIDS, global spending on HIV/AIDS in 2009 amounted to less than $16 billion, while 2010 funding needs exceeded $25 billion. More than 60 percent of people in need of anti-retroviral therapy drugs still can’t get them.
What’s next? The President’s State of the Union Address was silent on AIDS as both a domestic and international issue, and the climate of austerity surrounding the forthcoming fiscal year 2012 budget will leave little room for tackling global epidemics.
"If Obama wasn’t willing to fight for AIDS in a Democrat-controlled Congress, activists worry about what he is likely to do with the Republicans coming in complaining about deficits and foreign aid," said Health GAP policy analyst Brook Baker. He noted that even some of the sympathetic centrist conservatives, who supported PEPFAR under Bush, have now been "defeated by the tea partiers or fiscal conservatives. It’s going to be an uphill but winnable struggle."
AIDS on the Home Front
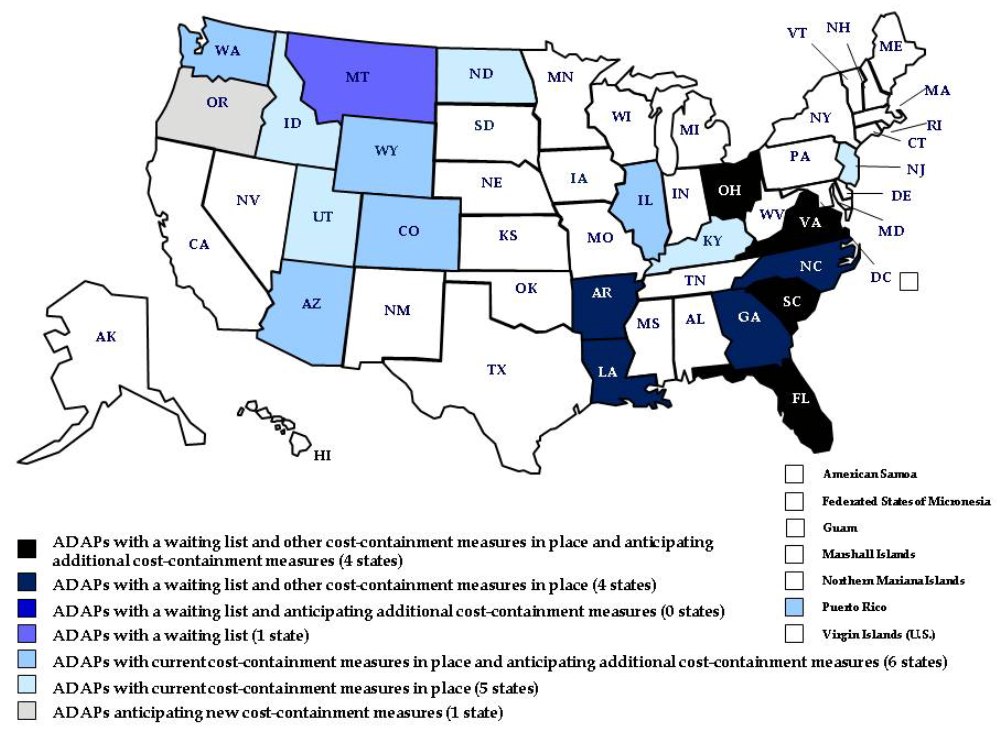
The struggle to deal with AIDS in U.S. communities is also lagging. Today, several thousand people are still on the waiting list for the AIDS Drug Assistance Program (ADAP), a 32 percent increase over a year, according to The Body. Much of this is due to state government rollbacks and freezes on programs to deal with budget deficits.
{kind=link}
The embattled healthcare bill contains several initiatives that could directly or indirectly strengthen access to treatment and prevention. But even those modest reforms are threatened by the Republican opposition, which could push decent medical care even further out of reach for people living with HIV and AIDS.
Phill Wilson, head of the Black AIDS Institute, wrote in a recent commentary that stigma and a lack of political momentum has fallen especially hard on Black communities:
When faced with discrimination, alienation and marginalization, people will not disclose their risk factors, use condoms, get tested for HIV, seek treatment or talk openly about HIV/AIDS.
The therapies, while effective, are very expensive (approximately $12,000 to $14,000 per year, not including the other costs of care). Without health insurance, many people living with HIV/AIDS cannot afford them. Many state-run, publicly funded AIDS drug assistance programs have waiting lists and are not able to accommodate everyone who needs these life-saving drugs.
Wilson is among those who have praised one major accomplishment of the Obama administration in the domestic epidemic: crafting the U.S.’s first comprehensive strategy for fighting HIV/AIDS. Advocates pushed hard to secure a commitment to create such a strategy from candidate Obama, and applaud the Office of National AIDS Policy for following through over the past two years. The question now is whether it will be implemented earnestly, including adequate funding. The hope is that the new National HIV/AIDS Strategy will allow resources to be targeted in the communities where the epidemic is most intense–among black Americans and, increasingly, in southern states.
Washington clearly has a stake in the global battle against HIV/AIDS, but how do we reconcile that urgent need with the chilling fact that black men in the nation’s capital experience rates of HIV that rival that of Sub-saharan Africa?
In reality, the trajectory of the U.S. AIDS crisis over the past generation ties directly into the global dynamics of the epidemic. Wherever the disease spreads, it sharpens patterns of gender, racial and socioeconomic inequality, and the most acute suffering takes place in communities historically excluded from the institutions that dictate how health resources are invested.
Thirty years on, the fight against AIDS can still claim many victories: International cooperation has yielded breakthroughs in treatment and prevention as well as medical research. The Obama administration removed funding restrictions on international programs that were based on anti-abortion and anti-prostitution ideologies.
All that has merely laid the groundwork for defeating the crisis. While AIDS will outlive the election cycle, the economic cycle, and perhaps even this generation, the U.S. commitment to combating the disease suffers from a shortsighted vision. Keeping up the fight shouldn’t force us to divide inadequate resources across interconnected needs, especially when we’ve already seen how far a little cooperation can take us.